

Dead Rats & Ghost Ships
Is Hantavirus the World's Next Pandemic — or the Next Pretext?


")
From the killing fields of Korea to a stricken cruise ship drifting off the African coast, a centuries-old rodent virus is suddenly making headlines worldwide. We examine the science, the system failures, and the unsettling questions that institutional silence refuses to answer.

On April 11, 2026, somewhere in the cold waters between Argentina and Antarctica, a 70-year-old Dutch man died alone aboard a cruise ship. His wife survived just long enough to be evacuated to Johannesburg — where she collapsed at the airport and died the following day. A third passenger, a German national, was dead within weeks. By early May, the world had a name for what killed them: the Andes strain of Hantavirus. And the world, still raw from COVID-19, began to ask the question it always asks now: Is this how it starts?
The MV Hondius — a Dutch-flagged expedition vessel carrying 147 passengers and crew from 23 nations — has become the most internationally scrutinised vessel since the Diamond Princess ran aground in pandemic history in 2020. Denied entry at Cape Verde, rebuffed by the Canary Islands, and now limping toward Tenerife with desperate passengers and an overwhelmed medical team aboard, the ship has become a floating symbol of the world’s fractured pandemic preparedness infrastructure.
But this story is bigger than one ship, one outbreak, and one virus. It raises questions that run deeper than virology — questions about institutional credibility, geopolitical timing, economic incentives, and the disturbing gap between what public health authorities say and what the data quietly reveals.
What Exactly Is Hantavirus?
Hantavirus is not new. It is not exotic. It has been quietly killing people for decades — largely in the shadows of poverty, agricultural labour, and ecological disruption, in places the world rarely notices.
The virus belongs to the Bunyaviridae family and comes in dozens of strains. Old-World variants — found across Europe and Asia — cause Haemorrhagic Fever with Renal Syndrome (HFRS), which attacks the kidneys. New-World variants — particularly those found in the Americas — cause Hantavirus Cardiopulmonary Syndrome (HCPS), which destroys the lungs. It is the latter category, and specifically the Andes strain, that now demands the world’s attention.

What makes the current outbreak so alarming is not any single number — it is the combination of factors converging simultaneously: a highly lethal strain known for rare human-to-human spread, a confined multi-national vessel, passengers who disembarked and dispersed across the globe before the outbreak was identified, and a geopolitical reflex to deny responsibility at every port.
“People come off and on at the ports. They don’t stay for the whole voyage... Many of the passengers were serious birdwatchers who had been on expeditions in South America.”
— Dr. Jill Blumberg, South Africa’s National Institute for Communicable Diseases
The Ghost Ship Timeline
To understand why public concern is justified, one must trace the anatomy of this outbreak with precision.

Is This the Next COVID-19?
Every time a novel or resurgent pathogen emerges, the pandemic comparison is inevitable. This time, the comparison is not merely alarmist — there are genuine structural parallels that demand sober analysis.
What they share: Both involve zoonotic origin (animal-to-human spillover). Both present with respiratory distress that can escalate to ARDS and death within days. Both have incubation windows long enough to enable silent international spread before diagnosis. And both have exposed exactly the same institutional fractures — slow notification, political denial, port refusals, and the tragic spectacle of sick people turned away from shores.
Where they fundamentally differ: Hantavirus is not a respiratory droplet disease in the way that SARS-CoV-2 was. Transmission requires direct contact with rodent material or, in the rare Andes strain case, prolonged close contact with an infected person. It does not aerosolise freely across rooms or through building ventilation systems. Its reproduction number (R0) even in documented human-to-human clusters is drastically lower than COVID-19’s R0 of 2–6 (or higher with Omicron).
“Even if transmission of ANDV were to happen from passengers evacuated from the ship, ANDV does not transmit easily, so it is unlikely that it would cause many cases or a widespread outbreak.”
— European Centre for Disease Prevention and Control (ECDC), May 6, 2026
WHO Director-General Dr. Tedros Adhanom Ghebreyesus has stated that the overall public health risk from hantavirus remains low, and officials have explicitly dismissed comparisons to a COVID-19-scale pandemic threat. The scientific consensus is that Andes virus, while deadly in individual cases, lacks the aerosol transmission efficiency required to fuel a global pandemic.
That said — and this matters — the efficiency of a pathogen is only one part of pandemic risk. The other part is institutional capacity, political will, and global equity in response. On all three counts, the world has already failed its first test with this outbreak.
Plandemic 2.0? The Conspiracy Ecosystem
It was inevitable. Within 48 hours of the MV Hondius story going global, the familiar machinery of pandemic conspiracy theory lurched into motion. Social media filled with claims of orchestrated timing, population control agendas, and bioweapon accusations. We examine the most prominent claims — fairly, rigorously, and without condescension.

The Economist’s Lens: Who Pays When the System Fails?
Strip away the conspiracy theories and the virological technicalities, and what remains is a story of institutional failure that has very clear economic and political dimensions — particularly for small and middle-income countries.
When Cape Verde and the Canary Islands refused entry to the MV Hondius, they were not being irrational. They were making a rational economic calculation rooted in COVID-era trauma: the cost of accepting a potentially infected vessel — in healthcare expenditure, tourism damage, and political fallout — vastly outweighs any humanitarian or international obligation, especially when wealthier nations and international institutions have repeatedly failed to compensate smaller countries for bearing disproportionate pandemic burdens.
This is the structural injustice at the heart of global pandemic response. The Caribbean knows this better than most. During COVID-19, small island developing states bore catastrophic tourism revenue losses while pharmaceutical manufacturers in wealthy nations raced to secure bilateral vaccine deals. The COVAX facility — meant to ensure equitable distribution — was chronically underfunded and consistently outmanoeuvred by wealthy nations hoarding supply.
“The president of the Canary Islands ‘cannot allow [MV Hondius] to enter’ — while the WHO says Spain has a moral and legal obligation to assist.”
— The Geopolitics of Pandemic Denial, in real time, May 2026
There is also the question of Argentina’s rising baseline infection rate — 101 hantavirus cases since June 2025, double the prior year. This increase has received almost no international attention. No emergency WHO declaration, no coordinated international response, no emergency funding. It took a cruise ship full of European and American birdwatchers dying in international waters to force the world to look.
This is how epidemics are born: not in laboratories and boardrooms, but in the indifferent arithmetic of which lives are deemed worth counting.
What the Science Actually Says About Pandemic Risk
Here is the honest, evidence-based assessment — stripped of both institutional reassurance and conspiratorial catastrophising.
The current outbreak is NOT a pandemic threat. The Andes strain has limited human-to-human transmission. The incubation window is long, but the transmission window is narrow. There is no evidence of mutation toward more efficient airborne spread. WHO’s low-risk classification is, on current evidence, scientifically justified.
The medium-term risk, however, deserves serious attention. RNA viruses mutate. Hantavirus is a negative-sense single-stranded RNA virus — the same broad family as influenza. Its documented history includes mortality rates between 36% and 60% in documented outbreak settings. Its global annual burden of 150,000–200,000 cases is almost certainly an undercount given the populations in which it concentrates: rural, agricultural, poor, and under-surveilled.
Climate change is not an abstraction in this story. Rising temperatures and changing precipitation patterns are expanding the ranges of rodent populations globally, increasing human-wildlife contact interfaces. The doubling of Argentinian hantavirus cases is consistent with these projections. If climate disruption continues at its current pace, “emerging zoonotic disease events” will not be anomalies — they will be the new baseline.
Georgia, Atlanta, and the Caribbean’s Open Door
On the surface, five American states monitoring a handful of asymptomatic former cruise passengers sounds like routine public health procedure. Dig one layer deeper, and a specific geography begins to matter enormously to the Caribbean.
Georgia is not just any American state. It is home to Hartsfield-Jackson Atlanta International Airport — the busiest airport in the world by passenger volume for over two decades running. Atlanta is Delta Air Lines’ primary hub, and Delta operates one of the most extensive Caribbean route networks of any North American carrier, with direct service to Grenada, Antigua, Barbados, Jamaica, Trinidad, Aruba, Curaçao, Puerto Rico, Saint Martin, the U.S. Virgin Islands, and beyond — often with multiple daily departures during peak tourist season.
")
This is not hypothetical catastrophising. This is the same arithmetic that allowed COVID-19 to spread from Wuhan to every continent within weeks — asymptomatic and pre-symptomatic travellers moving freely through aviation networks while public health institutions debated the appropriate response threshold.
The Andes strain’s documented ability to transmit human-to-human through sustained close contact means that an infected passenger sitting in a middle seat on a four-hour Delta flight from Atlanta to Grenada is not a zero-risk scenario. The risk is low — but it is not zero. And in a country like Grenada, where Maurice Bishop International Airport has no infectious disease isolation facility, where the general hospital has a finite ICU capacity, and where there is no domestic hantavirus diagnostic capability, the arrival of even a single symptomatic case would trigger a crisis that our system is simply not equipped to manage.
“California is one of five states monitoring people who previously traveled on the MV Hondius cruise ship, where a cluster of hantavirus cases turned deadly.”
— ABC7 Los Angeles, May 8, 2026
The European dimension compounds the picture. Several hundred thousand European tourists visit the Caribbean annually, with the UK, Germany, France, and the Netherlands — all countries with nationals directly affected by the MV Hondius outbreak — representing major visitor source markets for islands from Barbados to Sint Maarten to Turks and Caicos. Infected passengers are currently hospitalised in South Africa, the Netherlands, Germany, Saint Helena, and Switzerland — and a confirmed case emerged from a passenger who disembarked and returned to Switzerland before symptoms appeared. This is the model of silent spread that should worry Caribbean health authorities most.
The critical question Caribbean governments must ask — and are not visibly asking — is this: What is our protocol if a confirmed or suspected Andes hantavirus case steps off a plane at Grantley Adams, Piarco, V.C. Bird, or Maurice Bishop International?

What the Caribbean Must Do — And Do Now
This is not a moment for passive monitoring. The following is a concrete, policy-grounded preparedness framework that CARICOM health ministers and individual island health authorities should be implementing immediately.
1. Epidemiological Intelligence Sharing. CARPHA — the Caribbean Public Health Agency — must issue an immediate regional health alert, circulate the WHO case definitions for Andes hantavirus to all frontline clinical staff, and establish a real-time data-sharing protocol with CDC, PAHO, and ECDC. This should have happened on May 2. It has not, to public knowledge, happened yet.
2. Port Health and Airport Protocols. Every major Caribbean international airport and cruise port should implement a voluntary health declaration form specifically referencing hantavirus and travel to Argentina, Chile, or Uruguay since January 2026. This is low-cost, minimally disruptive, and epidemiologically sound.
3. Clinical Training. The clinical presentation of Andes hantavirus — fever, gastrointestinal distress, rapid progression to pneumonia and ARDS — can easily be mistaken for dengue, leptospirosis, or influenza in a Caribbean clinical setting. Emergency physicians and general practitioners across the region need a one-page clinical alert issued now, before a case presents.
4. Diagnostic Capacity. Currently, no Caribbean nation has confirmed in-country PCR diagnostic capability for Andes hantavirus. Samples would need to be couriered to CARPHA’s reference laboratory or to CDC Atlanta. In an outbreak context, that 48–72-hour diagnostic delay could cost lives. CARPHA must immediately identify the fastest specimen pathway and communicate it to all island health ministries.
5. Tourist Screening Partnership with Airlines. Caribbean governments, through their tourism ministries, should request voluntary compliance from Delta, American, British Airways, Condor, and other major carriers serving the region: enhanced passenger health declarations for travellers with recent South American travel history, and crew briefings on hantavirus symptom recognition. Airlines have shown willingness to cooperate on similar measures historically.
6. Public Communication — Without Panic. The Caribbean’s tourism-dependent economies cannot afford a repeat of the reputational catastrophe that health scares have historically triggered. The public communication task is precise: inform residents and tourists that the regional risk is low but that the region is prepared and vigilant. Silence is worse than calibrated transparency — it creates a vacuum that misinformation fills.
The Caribbean Dimension
Hantavirus is not currently endemic in the Caribbean. The rodent reservoir species — long-tailed pygmy rice rats and deer mice — are not native to our region. But endemicity is not the threat vector here. Importation is.
The Caribbean is an extraordinarily vulnerable region in the event of any new pandemic: high dependence on tourism which both imports and exports infectious disease; healthcare systems that remain under-resourced and under-staffed despite post-COVID pledges; geographic isolation that makes medical evacuation and supply chain management catastrophically difficult; and a geopolitical positioning that means we are typically the last to receive vaccines, antivirals, and diagnostics.
The MV Hondius scenario — a vessel denied entry at multiple ports, with sick passengers of 23 nationalities trapped aboard — is a scenario that Caribbean ports face with far less institutional capacity than Cape Verde or Tenerife. And yet there is a darker version of that scenario: not a ship announcing itself at anchor, but a passenger who doesn’t yet know they are infected, clearing customs at Hewanorra or Douglas-Charles or Crown Point, hugging a family member, staying in a shared villa, and then developing pneumonia five days later.
The window to prepare is right now. Not next week. Not after the first Caribbean case. Now!
Sources: World Health Organization Disease Outbreak News (DON-599), May 4–8, 2026 · European Centre for Disease Prevention and Control (ECDC) Risk Assessment, May 6, 2026 · Africa CDC Statement, May 5, 2026 · ABC News / ABC7 Los Angeles, May 8, 2026 · NBC News Multi-Country Tracking Report, May 8, 2026 · CNN Health Reporting, May 6–7, 2026 · TIME Magazine, May 7, 2026 · MV Hondius Hantavirus Outbreak — Wikipedia Live Summary, May 8, 2026 · Georgia Department of Public Health statement · Arizona Department of Health Services statement · U.S. CDC Level 3 Emergency Response Classification · Frontiers in Bioengineering and Biotechnology: “Biodefense Implications of New-World Hantaviruses,” August 2020 · WHO Hantavirus Fact Sheet (updated) · Argentine Ministry of Health epidemiological reports · Atlanta Journal-Constitution / Delta Caribbean Routes, 2025–2026 · U.S. CDC Hantavirus surveillance data, 1993–2023.
Editorial Note: This article presents a balance of confirmed scientific data, credible institutional reporting, and critical policy analysis. Claims labelled as conspiracy theories are examined on their evidentiary merits, not dismissed on cultural grounds. Caribbean Issues does not endorse bioweapon or depopulation narratives as explanations for this outbreak.

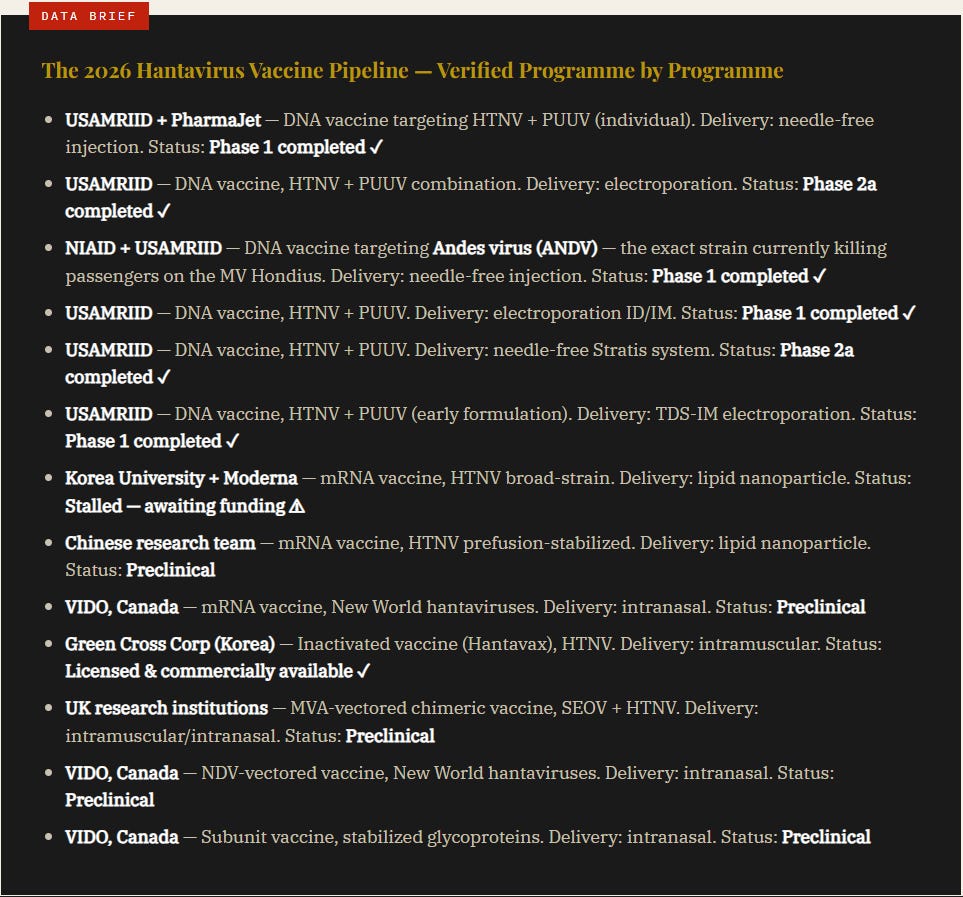
Thirteen Programmes Before One Outbreak: The Vaccine Pipeline Nobody Told You About
Here is a fact that no major news outlet covering the MV Hondius outbreak has placed front and centre — and it is perhaps the single most important contextual data point in this entire story.
As of 2026, there are thirteen documented hantavirus vaccine programmes in various stages of development worldwide. Seven are already in human clinical trials. Six use DNA vaccine platforms. Three use mRNA technology. One is already fully licensed and commercially available. And the lead developer across five of those thirteen programmes is not a pharmaceutical company. It is the United States Army.
Let that sink in. The U.S. National Institute of Allergy and Infectious Diseases — the same NIAID that Anthony Fauci led through the COVID-19 pandemic — partnered with the U.S. Army’s biological warfare research facility at Fort Detrick, Maryland, to conduct a Phase 1 human clinical trial of a vaccine specifically targeting the Andes virus. Results were published in the Journal of Infectious Diseases in January 2024. The trial enrolled 48 healthy adults across multiple dose cohorts. The vaccine was confirmed safe and produced a “robust and durable immune response.” They were ready.
And yet the world had no idea any of this existed until now.
“Force Protection — U.S. troops are frequently deployed to regions where hantaviruses are endemic. Biodefense — hantaviruses are considered potential biological warfare agents because they can be aerosolised from rodent droppings. Lack of Commercial Interest — because natural outbreaks are relatively rare, private pharmaceutical companies showed little interest. The military filled this gap.”
— Documented rationale for U.S. Army hantavirus vaccine research, tracing to Korean War, 1950s
The U.S. military’s interest in hantavirus is not new or sudden. It dates to the Korean War, when over 3,000 American and UN troops were stricken by a mysterious haemorrhagic fever later identified as Hantaan virus — a close relative of the virus now killing people at sea. USAMRIID has conducted research to develop medical countermeasures against biological threats and emerging diseases since 1969. Hantavirus has been on its target list for decades — formally classified alongside anthrax, plague, Ebola, and Marburg in the military’s biodefence priority matrix.
The United States government was awarded a hantavirus vaccine patent as early as March 1997 — U.S. Patent 5,614,193 — with lead inventor Connie Schmaljohn, a prominent USAMRIID virologist at Fort Detrick. The assignee: the United States of America, as represented by the Secretary of the Army.
That is nearly thirty years of documented state-level development of hantavirus countermeasures, classified under the military’s biodefence remit, progressing quietly through the pipeline — while the rest of the world learned about hantavirus only when it appeared on a cruise ship in 2026.
The Moderna Angle: Profit Architecture in Plain Sight
In September 2023, Korea University’s Vaccine Innovation Center and Moderna signed a research and development agreement under Moderna’s mRNA Access initiative to develop a broad-strain hantavirus mRNA vaccine. Experimental doses prevented hantavirus infection in mice, confirmed in February 2025. But human clinical trials have been on hold for more than a year while researchers waited to be selected for a national project — stalled for want of between €6.5 million and €13 million.
To contextualise that number: Moderna booked revenues of $18.5 billion in 2021 and $19.3 billion in 2022, mostly from Spikevax COVID-19 vaccine sales. The company could fund the entire hantavirus clinical trial programme from the change in its executive compensation budget. It chose not to. The programme sat dormant — until a cruise ship outbreak created the precise conditions under which vaccine development funding becomes politically and commercially irresistible.
This is not necessarily sinister. It is, however, a precise demonstration of how the pharmaceutical industry’s profit architecture operates: neglect endemic disease that disproportionately kills the poor, wait for a high-visibility outbreak involving wealthy nationals, then mobilise. Experts say hantavirus vaccine efforts have repeatedly stalled in part because outbreaks tend to occur sporadically and disproportionately affect poorer countries where there is less incentive for drugmakers to invest.
The MV Hondius changed the calculus. Watch the pipeline accelerate now.
⬛The Caribbean Issues Verdict — Updated May 10, 2026
Let us be precise about what the vaccine pipeline data proves — and what it does not.
What it proves: The United States Army, NIAID, Moderna, academic institutions in Canada, South Korea, China, and the United Kingdom were all engaged in active, funded, documented hantavirus vaccine research before a single passenger on the MV Hondius fell ill. Thirteen programmes. Seven in human clinical trials. One — targeting the exact Andes strain now killing people at sea — completing Phase 1 trials and publishing peer-reviewed results in January 2024. The U.S. government holds a hantavirus vaccine patent dating to 1997. Fort Detrick has classified this virus as a military biodefence priority for over seventy years. None of this was secret. All of it was publicly available in scientific literature and government databases. None of it was reported to the public until an outbreak forced the question.
What it does not prove: Deliberate release. The depopulation agenda narrative. A coordinated “Plandemic 2.0” operation. The scientific, epidemiological, and intelligence evidence does not support those conclusions. The index case has been identified — Leo Schilperoord, a 70-year-old Dutch ornithologist whose four-month travel route through Chile, Uruguay, and Argentina prior to embarkation has been mapped and is being rodent-sampled by Argentine authorities. This is how natural zoonotic spillover events look. As of now we don’t now that the virus arrived from a laboratory. It’s attributed to have arrived from a field mouse.
What demands serious interrogation: The gap between institutional foreknowledge and public preparedness is not explainable by incompetence alone. The U.S. military knew hantavirus was dangerous enough to spend decades developing countermeasures — and classified it alongside anthrax and plague in its biodefence priority matrix. NIAID co-funded a Phase 1 trial of an ANDV-specific vaccine, published January 2024. And yet Argentina’s doubling infection rate received no emergency international response. The WHO issued no proactive alert. The Caribbean has no diagnostic capacity for this virus. Moderna’s mRNA programme sat stalled for want of €13 million while the company held billions in post-COVID revenues. The political economy of pandemic preparedness is not conspiracy — it is structural. Institutions that profit from outbreak response have rational incentives not to prevent outbreaks quietly.
The Caribbean’s specific position: We sit at the terminus of one of the world’s most active aviation corridors. Passengers from Georgia, Arizona, California — states now under active federal surveillance — board Delta flights to Grenada, Barbados, Antigua, and beyond every single day without screening, without declaration requirements, and without any regional protocol for what happens if one of them arrives febrile. Our health ministries have issued no alert. CARPHA has issued no regional guidance. The hantavirus diagnostic pathway from Maurice Bishop International Airport runs through Atlanta. We are, in the most literal epidemiological sense, downstream of this outbreak — and we are not prepared.
The verdict: This is may not be Plandemic 2.0. It is may not be a depopulation conspiracy. It is something more troubling and more verifiable: a global public health architecture that invests in countermeasures for known threats while keeping those investments hidden from the populations most exposed to those threats — and that is structurally configured to respond to outbreaks only when the right people start dying. The pipeline was built. The knowledge existed. The warning signs were visible. The Caribbean was not included in any of it.
Watch the Andes. Watch the rats. Watch the planes from Atlanta. Watch the vaccine contracts that are, even now, being quietly expedited. And above all — demand that our governments stop being the last to know and the last to be protected.